 | Oral contrast: Generally not required for adrenal protocols. |
|
Adrenal nodule characterization
|
The goal of the exam is to determine whether an adrenal nodule is (1) a benign adenoma or (2) something more worrisome such a metastasis, pheochromocytoma, or adrenal cortical carcinoma.
1. Noncontrast images of ABDOMEN ONLY
| ● |
If noncontrast attenuation of the nodule measures <10 HU, it is diagnosed as a lipid-rich adenoma, and no further imaging is necessary. |
| ● |
However, for attenuation values >10 HU, additional venous and delayed phases are obtained to calculate % washout. |
2. Venous phase of ABDOMEN ONLY
3. Delayed phase (15 min) of ABDOMEN ONLY
 Calculating washout Calculating washout

| ● |
Rapid contrast washout (relative washout >40% and absolute washout >60%) usually indicates that the lesion is an adenoma.
| ○ |
Exceptions: Pheochromocytomas and metastases from RCC or HCC can also washout rapidly, similar to adenomas. |
|
| ● |
Slower contrast washout suggests that the lesion is not an adenoma. |
|
|
 Pitfall Pitfall
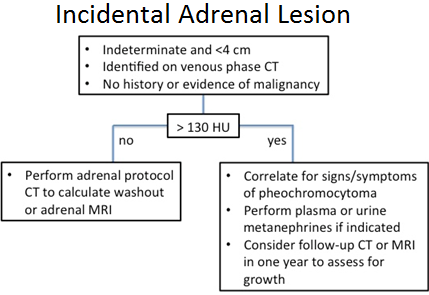
Many pheochromocytomas, particularly more vascular lesions (>130 HU on venous phase), will demonstrate rapid washout similar to adenomas. Accordingly, the following algorithm has been developed [1]:
Illustrative case: Pheochromocytoma mimics adenoma at adrenal washout CT. Venous (A) and delayed phase (B) axial IV contrast-enhanced CT show a 1.3 cm right adrenal mass (arrow) that measured 42 HU on non-contrast phase (not shown), 178 HU on venous phase, and 64 HU on 15 minute delay phase, meeting both APW and RPW washout criteria for adenoma. A mass that enhances > 130 HU cannot be assumed to be an adenoma regardless of washout pattern, and washout CT will not be helpful to distinguish adenoma from pheochromocytoma.
(A) Venous phase |
(B) Delayed phase |
|
1. Northcutt B et al. Adrenal adenoma and pheochromocytoma: Comparison of MDCT venous enhancement levels and wash-out characteristics. JCAT. In press.
|
|
| Evaluating for adrenal adenoma in setting of known hormone hypersecretion |
1. Noncontrast images of ABDOMEN ONLY
| ● |
If a hypodense adrenal nodule measuring <10 HU is identified, no additional imaging is necessary. |
| ● |
Otherwise, add a venous phase to help improve detection of small adrenal nodules (or to characterize a hyperattenuating adrenal nodule). |
2. (If necessary) Venous phase of ABDOMEN ONLY
| ● |
If no adrenal nodule → no additional imaging. |
| ● |
If adrenal lesion present → obtain delayed phase to calculate % washout |
3. (If necessary) Delayed phase (15 min) of ABDOMEN ONLY
|
| Biochemically diagnosed pheochromocytoma |
90% of pheochromocytomas arise in the adrenals. The remaining 10% arise along the sympathetic chain anywhere from the neck to the urinary bladder. Most of these extra-adrenal pheochromocytomas are located in the abdomen or pelvis, with common locations being the paraaortic region and urinary bladder.
Therefore, when searching for a biochemically diagnosed pheochromocytoma, start with dual-phase CT of the abdomen and pelvis:
1. Arterial phase of abdomen and pelvis
a. Look for heterogeneous, arterially enhancing mass
b. Look for hypervascular metastases
|
2. Venous phase of abdomen and pelvis
|
a. Some pheochromocytomas have greater enhancement on venous phase
|
|
If abdominal CT is negative, consider:
| ● |
CT of the chest and neck with arterial and venous phases |
| ● |
Whole body MRI |
| ● |
I-123 MIBG or In-111 pentetreotide scan |
| ● |
FDG PET/CT |
|
FAQ 
| Q: |
Is it safe to give IV contrast to patients with pheochromocytomas? |
| A: |
Yes. Premedication with alpha or beta blockers is NOT necessary (although patients who are already on alpha or beta blockers should take their medications). While it was previously thought that iodinated contrast could precipitate hypertensive crisis in patients with pheochromocytomas, multiple studies have now shown that this is not the case [1-3].
|
|
1. Baid SK, Lai EW, Wesley RA, Ling A, Timmers HJ, Adams KT, et al. Brief communication: Radiographic contrast infusion and catecholamine release in patients with pheochromocytoma. Ann Intern Med. 2009 Jan 6. 150(1):27-32.
2. Bessell-Browne R, O'Malley ME. CT of pheochromocytoma and paraganglioma: Risk of adverse events with IV administration of nonionic contrast material. AJR Am J Roentgenol. 2007 Apr. 188(4):970-4.
3. Mukherjee JJ, Peppercorn PD, Reznek RH, et al. Pheochromocytoma: Effect of nonionic contrast medium in CT on circulating catecholamine levels. Radiology. 1997;202(1):227-31.
|
|
 KRISTIN PORTER, MD, PHD PAMELA JOHNSON, MD
KRISTIN PORTER, MD, PHD PAMELA JOHNSON, MD