Adult Enterography
|
Purpose
|
To evaluate the bowel for intraluminal and extraluminal abnormalities. Primary indications include evaluation for active Inflammatory Bowel Disease and its complications. Less common indications include evaluation for celiac disease, small bowel obstruction and small bowel neoplasm.
|
Patient preparation
|
Goal is optimal distension of small bowel.
- Light diet evening prior to exam
- NPO 6 hours prior to exam
- Reduces food residue and debris
- No carbonated beverages
- VoLumen 1350 mL total 1 hour before exam
- Distends bowel and provides intraluminal contrast
- 450 mL First 10 mins
- 450 mL 10 mins after first dose
- 450 mL 10 mins after second dose
- 0.02 mg/kg IM Glucagon immediately prior to study
- Antiperistaltic agent
- Not administered in patients with diabetes
- Prone positioning
- Separates bowel loops
- May reduce motion
- Contraindicated in patients with stomas, fistulas, large hernias, intolerance, etc.
 Pearls regarding VoLumen Contrast
VoLumen: distends bowel, which is essential to this examination, as collapsed loops hide lesions or mimic disease Pearls regarding VoLumen Contrast
VoLumen: distends bowel, which is essential to this examination, as collapsed loops hide lesions or mimic disease
- Biphasic Enteral Contrast
- Low signal on T1: Bowel wall/masses pre-and post-contrast
- High signal on T2: Endoluminal abnormalities
|
|
Common sequences
|
Scout localizer images:
|
3 planes, 5 images. FLASH (spoiled GRE)
|
Coronal/Axial T2 True FISP
|
Primarily for anatomic overview; however, areas of edema, bowel wall thickening, luminal dilation, and fibrofatty proliferation may be identified.
|
Coronal/Axial T1 Vibe (pre-and post- 0.1mmol/kg gadolinium contrast)
|
- Gadolinium Contrast
- Improves detection of inflammation
- Active versus inactive disease
- Improves detection of fistula and abscesses
- Helps characterize strictures
- Enhances detection of extraenteric findings
- MRE can still be beneficial in patients who cannot receive gadolinium contrast
|
Coronal (thick/thin) T2 SSFSE
|
Covers entire small bowel and colon. These images are akin to the overhead images acquired in fluoroscopic small bowel series with small bowel follow through. They allow global evaluation of the small bowel for evidence of stricture or obstruction. These images may also provide another look at fibrofatty proliferation and dilated vasa recta.
|
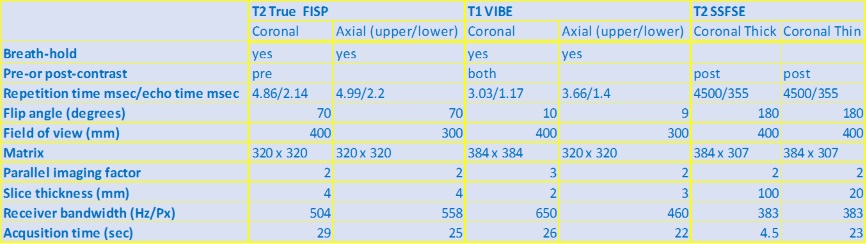
Sequence Details for 1.5T MR Imaging with abdominal coil:
|
Illustrative cases
|
|
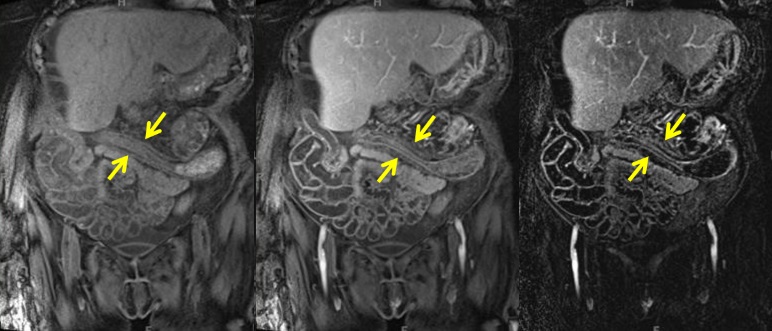
Case 1: Crohn's Disease
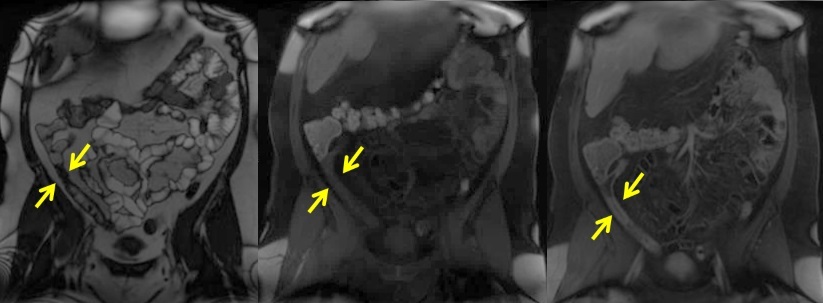
T2-weighted coronal image and T1-weighted pre- contrast and post-contrast images demonstrate terminal ileum mural (wall) thickening with hyperenhancement and suspected stricture of the most distal ileum (yellow arrows).
|
|
Case 2: Crohn's Disease
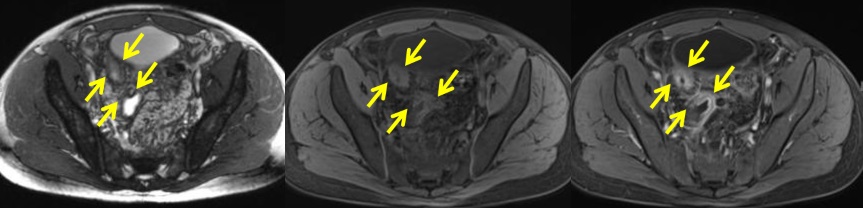
T2-weighted axial image and T1-weighted pre- contrast and post-contrast images demonstrate multiple segments of small bowel with bowel wall thickening and hyperenhancement (yellow arrows), compatible with severe active Crohn's disease.
|
|
Case 3: Crohn's Disease
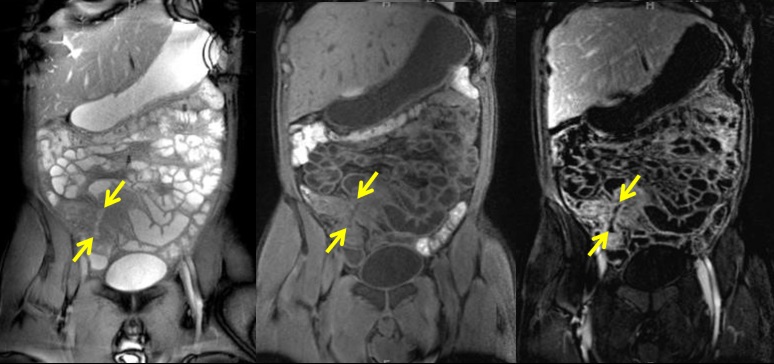
T2-weighted coronal image and T1-weighted pre- contrast and post-contrast images demonstrate a conglomerate of abnormal bowel loops in the right lower abdomen with mural wall thickening, hyperenhancement, and surrounding mesenteric inflammatory changes, consistent with acute inflammation. Enteroenteric fistula is seen (yellow arrows).
|
|
Case 4: Ulcerative Colitis
T1-weighted coronal pre-contrast, post- contrast and subtraction images in a patient with history of ulcerative colitis demonstrate featureless transverse colon (yellow arrows) with loss of haustra and thickened bowel wall. Mural fatty replacement compatible with long-term history of prior colitis. No hyperenhancement of the thickened bowel wall to suggest active inflammation.
|
|
 KRISTIN PORTER, MD, PHD PAMELA JOHNSON, MD
KRISTIN PORTER, MD, PHD PAMELA JOHNSON, MD